Coronary heart disease is a major cause of death and disability in developed countries including Malaysia. Stent implantation has become an efficacious treatment for a culprit lesion vessel of the coronary artery. However, 10%–20% restenosis is still an important complication that restricts the clinical safety and efficacy of drug-eluting stents. In-stent restenosis may lead to the recurrence of major cardiovascular adverse events, including angina pectoris, acute myocardial infarction, and even sudden cardiac death. These events are currently serious problems that occur after coronary stent implantation. Malaysia Clinical physicians face a difficult choice for in-stent restenosis treatment. Recent studies indicate that a drug-coated balloon has promising clinical efficacy similar to the drug-eluting stents for treating coronary in-stent restenosis.
Coronary heart disease (CHD) has become the “first killer” that endangers human health. CHD weakens the heart muscle and leads to heart failure and arrhythmias. Percutaneous coronary intervention (PCI) helps in recovering the coronary flow and has become an efficacious treatment for revascularization of the blocked coronary artery.
PCI includes percutaneous transluminal coronary angioplasty (PTCA), stent implantation, and drug-coated balloons (DCBs). The rapid development of stent bioengineering technology and drug carriers has improved the safety and efficacy of stent treatment. Compared with PTCA in which restenosis occurs at the rate of up to 50%, the rate of in-stent restenosis (ISR) in patients with drug-eluting stents (DESs) decreased significantly; however, 10%–20% restenosis is still a major complication, restricting the clinical safety and efficacy of DESs. ISR may lead to a recurrence of major adverse cardiovascular events (MACEs), including angina pectoris, acute myocardial infarction, and even sudden cardiac death.
No stents were available in the early 1970s. Although balloon dilation could reduce coronary artery stenosis, owing to the property of elastic recoil and intimal tear of the vessel wall, vascular restenosis may reoccur again. The vascular retraction rate after simple balloon dilatation angioplasty was as high as 30% to 60% 3 to 6 months postoperatively. In the 1980s, the emergence of bare-metal stents (BMSs) led to a 30% incidence of restenosis. Recent DESs combined with antiproliferative drugs, such as paclitaxel and sirolimus, reduced the incidence of ISR to less than 10%. Although the incidence of ISR is gradually declining, still it cannot be completely prevented.
Although ISR is much less common with the use of DESs than BMSs, the number of stents implanted in interventional practice means that the treatment of ISR remains an important clinical challenge. Malaysia Clinical physicians face a difficult choice for ISR treatment. Accumulative evidence indicates that drug-coated balloon (DCB) angioplasty, as a similar new DES treatment for coronary ISR, have been considered as an alternative option for treating coronary ISR, avoiding repeated stenting after ISR that leads to expose the patient to cost and risk of a prolonged DAPT. Therefore, in this study, we highlight the progress of coronary intervention and the use of DCBs in the treatment of ISR.
In-Stent Restenosis
ISR is defined as new proliferative lesions of more than or equal to 50% of the lumen diameter, involving either the stent segment or adjacent 5 mm segments on both sides of the stent by coronary angiography (CAG). After a successful PCI procedure, coronary stents can fail to maintain vessel patency as a result of either restenosis or thrombosis; restenosis is a gradual re-narrowing of the stent segment that mostly occurs between 3 and 12 months after stent implantation. Restenosis usually presents as recurrent angina but can present as an acute myocardial infarction in approximately 10% of patients. Restenosis can usually be managed by repeat percutaneous revascularization.
The patterns of ISR lesions can be divided into two broad categories: focal—lesions localized within the stent that are <10 mm in length are said to be Type I lesions and can be focal single or focal multiple—and diffuse—diffuse lesions are >10 mm in length and may or may not be confined to the edges of the stent. Type II diffuse lesions are confined to the stent edges, Type III diffuse lesions overhang the stent edges, and Type IV diffuse lesions completely occlude the stent.
Pathology of In-Stent Restenosis
Restenosis was understood to be the result of exuberant smooth muscle cell proliferation and macrophage infiltration inside the stent. Arterial vessels are abundant in elastic fibers that provide vessels with recoiling properties after they are distended by any means. Recoiling occurs within seconds to minutes after the procedure. ISR is mainly caused by neointimal hyperplasia, which occurs in response to local arterial injury sustained during PCI, leading to complex inflammatory and reparative processes. Neointimal hyperplasia first develops as damage to the arterial wall, followed by platelet aggregation at the site of the injury, recruitment of inflammatory cells, proliferation and migration of vascular smooth muscle cells, and collagen deposition.
Deployment of a stent at the lesion site requires inflation of a balloon apposing it in approximation with the vessel wall, thereby stretching the plaque and vessel wall layers. Intima and media tears give rise to a complex inflammatory response; this phenomenon, via multiple mechanisms, can lead to excessive neointimal proliferation, thereby decreasing the minimal luminal diameter (MLD). Neointimal proliferation is a process by which smooth muscle cells and myofibroblasts are mobilized from the media and adventitia of vessel walls, respectively. Redistribution and overgrowth of smooth muscle cells on stent struts cause luminal loss. This process takes months and is almost complete at 6 months; after 6 months, there is a shift in the cellular distribution that causes the collagen and proteoglycan matrix to become the major component of the growing lesion. Interestingly, this shift in cellularity leads to a relative decrease in late luminal loss as a result of the shrinkage in the lesion width. This process occurs from 6 months to 3 years.
Evidence-Based Practice of Treating ISR Using DCBs
The treatment options for ISR include PCI with DESs, DCBs, or PTCA. DCBs and second-generation DESs were equally effective in treating coronary ISR, according to a new systematic review and meta-analysis. Paclitaxel and rapamycin analogues have been proven successful in preventing neointimal hyperplasia and ISR. Different characteristics of these agents may affect their clinical efficacy. Paclitaxel is a diterpenoid compound isolated from the Pacific yew tree. Due to its high lipophilic characteristics, paclitaxel promotes rapid cellular uptake. Paclitaxel inhibits mitotic progression and cell proliferation in the G0-G1 and G2-M phases of the cell cycle. Sirolimus, a rapamycin analogue, forms a complex with the cytosolic immunophilin, FK506 binding protein-12, which in turn blocks the activation of the cell-cycle-specific kinase, mammalian target of rapamycin (mTOR). mTORC1 regulates translation, transcription, cell cycle progression, and survival through the phosphorylation of p70 56 kinase and 4E-BP1.
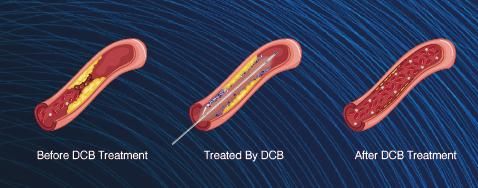
Drug-coated balloon angioplasty is similar to plain old balloon angioplasty, with the addition of an antiproliferative medication coating on the balloon, which helps reduce and prevent restenosis. The drug coating comprises an active drug and a carrier. The active drugs are paclitaxel and rapamycin. The current DCB prevents the premature release of drugs before the balloon catheter is positioned at a target site and promotes the drugs that are quickly released from the surface of the balloon and absorbed by the target tissue. DCBs were used to treat coronary ISR. Recent clinical trials on DCBs are summarized in Table 1. Scheller et al. reported that a paclitaxel-eluting balloon (PEB) significantly reduced the incidence of ISR compared with POBA in porcine coronary arteries. In a study by Scheller et al., the LLL of PEBs was significantly lower than that of POBA by CAG after 6 months of follow-up; the incidences of ISR and MACEs were also significantly lower than that of POBA. Furthermore, long-term follow-up results also showed a good therapeutic effect with PEBs.
Should you need any further information, please do not hesitate to contact contactus@laprimamedical.com.

Table 1
Source: Zhang DM, Chen S. In-Stent Restenosis and a Drug-Coated Balloon: Insights from a Clinical Therapeutic Strategy on Coronary Artery Diseases. Cardiol Res Pract. 2020 Oct 25;2020:8104939. doi: 10.1155/2020/8104939. PMID: 33163230; PMCID: PMC7605950.